Blast injuries
Injuries that were rarely seen beyond the battlefield are slowly starting to show up in the civilian arena. With the ever increasing risks of terrorist attacks worldwide the potential for casualties related to explosions are also at risk of increasing. Yet in the UK few EMS providers have had experience in dealing with these types of injury
A blast injury occurs from the result of a direct or indirect exposure to an explosion. Blast injuries occur due to overpressure occurring as a result of the detonation of high explosives. These injuries are compounded when the explosion occurs in a confined space.
Classification
Blast injuries are divided into four classes: primary, secondary, tertiary, and quaternary.
- Primary blast injury is a direct result of the overpressurization wave's impact on the body. These injuries occur mainly to the gas-filled organs of the auditory, pulmonary, and gastrointestinal systems. (Internal injuries are frequently unrecognized and their severity underestimated).
- Secondary blast injuries result from flying debris and device fragments propelled by the explosion leading to penetrating ballistic or blunt force injuries.
- Tertiary blast injuries occur as a result of individuals being thrown by the blast wind. Victims may tumble along the ground or be thrown through the air and strike other objects with resultant blunt or penetrating trauma, including bone fractures and coup contre-coup injuries.
- Quaternary blast injuries are defined as any explosion-related injury or illness not due to any of the above such as flash burns, crush injuries and respiratory injuries.
Blast Lung Injury (BLI)
BLI is a major cause of morbidity and mortality for blast victims both at the scene and among initial survivors. The 'Blast' from an explosive device sends out a shock wave which impacts on the lungs and results in tearing, haemorrhage, contusion, and oedema which results in a ventilation/perfusion disassociation.
Possible Signs and Symptoms in the Absence of any Visible Injury
- Dyspnoea
- Haemoptysis
- Cough
- Chest pain
- Tachypnea
- Hypoxia
- Cyanosis
- Apnoea
- Wheezing
- Decreased breath sounds
- Haemodynamic instability
Injuries associated with early mortality are:
- Multiple trauma
- Head trauma
- Thoracic injury
- Abdominal injury
General Management Techniques
Recognition of specific hazards associated with a suspected terrorist bombing, such as secondary devices and structural instability.
A METHANE radio call to your dispatcher in the event of an explosion in a highly populated area
Consider HART/HEMs deployment
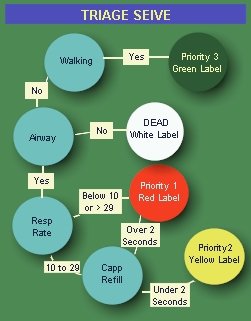
TRIAGE
Administer high concentration of O2 (As per O2 Guidelines), Assisted ventilations if needed (Positive pressure ventilation may increase the risk of alveolar rupture and air embolism in presence of Blast Lung Injury, BLI), Patient positioning. as much history as possible should be obtained. *Important historical information includes distance from the explosion; whether open, closed, or semiconfined space*
Continually monitor patient condition
Priority ASHICE
Smooth and rapid Time Critical journey to appropriate hospital facility (Major Trauma Unit or Trauma unit - Use local trauma decision trees to help your decision)
Professional handover to hospital staff
Other Reading
http://www.bt.cdc.gov/masscasualties/blastlunginjury_prehospital.asp
http://en.wikipedia.org/wiki/Blast_injury
http://en.wikipedia.org/wiki/Triage
http://www.sempermax.com/ied_injuries_145.html